
The role of the Dietitian
The dietitian will be involved from an early stage in order to help prevent malnutrition or from malnutrition worsening. If possible the dietitian will become involved in the patients care as soon as the patient is admitted to hospital.
If a patient is admitted to hospital several days before their operation and they have experienced weight loss, help and advice can be given to build the patient up, which can help with recovery after surgery.
The dietitian will carry out a full assessment at the initial consultation; this will also include asking questions in order to gain a picture of the weight history and current oral intake of the patient.
The dietitian will assess weight, weight changes, body mass index (BMI), current oral intake, age and diagnosis to calculate daily nutritional requirements for calories, protein and fluid for the patient being assessed.
The patient’s current oral intake is then assessed, if this falls short of their individual requirements the patient will be encouraged with high calorie and high protein foods, extra snacks, little and often to increase their calorie and protein intake. Nutritional supplements may also be offered if the dietitian feels the patient requires them.
Malnutrition
Patients with head and neck cancers can experience pain on eating, suffer with mouth ulcers and have difficulties swallowing (dysphagia), which can prevent a normal diet from being consumed. Many patients may lose weight as a result of this and are admitted to hospital already malnourished.
Nutritional status can be compromised further during hospital stay as surgical procedures may restrict oral intake or require patients to be ‘nil by mouth’ for prolonged periods of time.
The nursing staff will refer all head and neck oncology patients on admission to the hospital to the dietitian for a full nutritional assessment.
Nutritional Support
Nutritional Supplements are given in addition to meals to help meet the patient’s nutritional requirements. Supplements are not a meal replacement and should be taken in between mealtimes.
A variety of supplements are available to suit different needs, for example milkshakes, juice drinks, soups and desserts. The majority are enriched with energy, protein, vitamins and minerals which the patient may not be able to get from their diet if their intake is restricted.
If supplements are advised by the dietitian, the dietitian will discuss with the patient the most suitable supplement to meet their needs.
Artificial nutrition support
Patients who are unable to meet their nutritional requirements with nutritional supplements or for those who are nil by mouth post operatively artificial nutrition support may be required (also known as enteral feeding or tube feeding). This is where the patient is fed directly into the stomach or intestine through a tube. The two types most commonly used are Nasogastric (NG) and Percutaneous Endoscopic Gastrostomy (PEG) feeding.
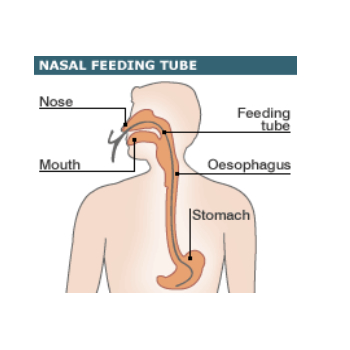
Nasogastric feeding (NG)
An NG tube is placed through the nose and down into the stomach, by either a staff nurse or doctor on the ward. The patient may have an NG tube placed during theatre. The patient may have to be fed through the NG tube in the first few days or weeks immediately after surgery when the patient is unable to eat for a short period of time. An NG tube is only temporary and can be removed easily. Once the patient is able to take oral diet the dietitian will assess the need for the NG tube and this will be removed when the patient is able to meet nutritional requirements orally.
Percutaneous Endoscopic Gastrostomy feeding (PEG)
This may be placed prior to surgery if the patient will not be able to eat post operatively for more than one month. A PEG may also be placed in those who need radiotherapy after discharge from hospital as the treatment can leave the throat and mouth area inflamed and sore making eating extremely difficult.
A PEG tube is placed by forming a hole from the skin into the stomach (called a stoma); a tube is placed through this hole which delivers feed, fluid and medication into the stomach.
This procedure is carried out endoscopically where the patient is sedated and will not be able to remember afterwards. The dietitian will decide on a suitable feed and the volume required meeting the patient’s individual needs. The feeding tube can be removed if no longer required. The dietitian and medical team will decide upon this if the patient is able to maintain their weight over a long period of time without the PEG feed. When the tube is removed the hole will close over.

What to expect after being discharged from hospital
If the patient is going home on a PEG feed or nutritional supplements one week’s supply will be provided by the nursing staff before going home. Those patients that require PEG feeding at home will be given full training before discharge on how to set up the equipment by a specialist nurse. The special feed and equipment will be provided on a monthly basis from the feeding company via a GP prescription. Full information regarding the feeding regime, supply of feed and equipment will be provided by the dietitian on the ward. The nutritional supplements are also available on prescription and these can be collected from the chemist.
Texture modified diets
Head and neck cancer patients may experience difficulty or discomfort when swallowing food or drink. This may be a short-term difficulty or may require some support over a longer period of time.
After surgery patients can have difficultly swallowing and a speech and language therapist should advise you on the best consistency of food and drinks you may need.
The dietitian will assist on advising a well balanced diet to meet your nutritional requirements depending on the advised consistency of your diet. The speech and language therapist will advise on the safest consistency of foods which may include pureed, fork/mashed or soft diet. Drinks may need to be thickened to certain consistencies to make them easier or safer to swallow such as ...
Thin fluid, naturally thick fluid or thickened fluid which may need thickener added. Puree diet – should be blended into a smooth paste with no lumps, it should be thick enough to fall off a spoon slowly but not pour off it; pureed food should not need any chewing.
Fork mashed –consists of moist foods which can be mashed into small soft lumps with a fork. Very little chewing is required. Soft diet – should consist of moist food which is easy to chew. Some foods may need to have gravy or a sauce with them to make them easier to swallow.
After discharge from hospital the patient will be followed up by a community dietitian or at Aintree ECC HN OPD by the HN Dietitian. They will carry out similar assessments as those on the ward, such as monitoring the patient’s weight and checking if there are any problems with the PEG feed or nutritional supplements. If the patient continues to lose weight once at home, the feed may be changed in order to maintain their weight. For those who are able to eat, their diet will be assessed to determine if they are taking enough energy and protein. Following this the supplements may either be increased or decreased as required. If the patient requires Radiotherapy/Chemotherapy as part of their treatment they will also be seen by a dietitian at Clatterbridge Centre for Oncology.
Dietician
Rachel Skelly